
Clinical Pharmacogenetics of Cytochrome P450-Associated Drugs in Children


Abstract
:1. Introduction
2. Results
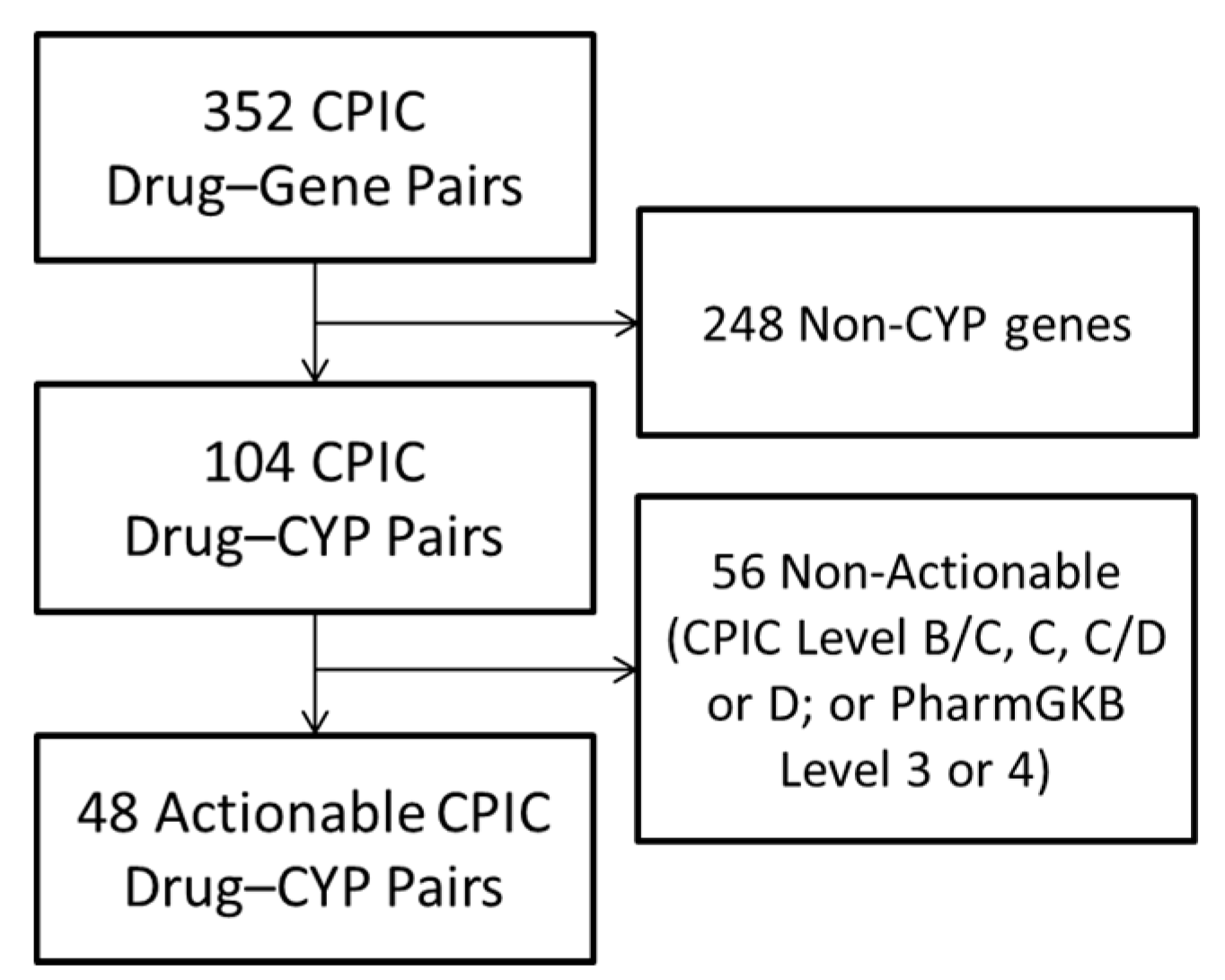
2.1. CYP-Associated Drugs with High Levels of Evidence
2.2. Pediatric Exposures to 41 CYP-Associated Drugs
2.3. Review of the Literature Supporting Drug–CYP Interactions for Drugs Commonly Used in Children
2.3.1. Ondansetron
2.3.2. Oxycodone and Codeine
2.3.3. Omeprazole and Lansoprazole
2.3.4. Sertraline
2.3.5. Amitriptyline
2.3.6. Citalopram and Escitalopram
2.3.7. Risperidone
3. Discussion
4. Materials and Methods
4.1. Identification of CYP-Associated Drugs with High Levels of Evidence
4.2. Determining the Pediatric Exposures to CYP-Associated Drugs
4.3. Literature Review for Drug–CYP Interactions in Children
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Williams, J.A.; Hyland, R.; Jones, B.C.; Smith, D.A.; Hurst, S.; Goosen, T.C.; Peterkin, V.; Koup, J.R.; Ball, S.E. Drug-drug interactions for UDP-glucuronosyltransferase substrates: A pharmacokinetic explanation for typically observed low exposure (AUCi/AUC) ratios. Drug Metab. Dispos. 2004, 32, 1201–1208. [Google Scholar] [CrossRef] [PubMed]
- Shuldiner, A.R.; Relling, M.V.; Peterson, J.F.; Hicks, J.K.; Freimuth, R.R.; Sadee, W.; Pereira, N.L.; Roden, D.M.; Johnson, J.A.; Klein, T.E.; et al. The Pharmacogenomics Research Network Translational Pharmacogenetics Program: Overcoming challenges of real-world implementation. Clin. Pharmacol. Ther. 2013, 94, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Pulley, J.M.; Denny, J.C.; Peterson, J.F.; Bernard, G.R.; Vnencak-Jones, C.L.; Ramirez, A.H.; Delaney, J.T.; Bowton, E.; Brothers, K.; Johnson, K.; et al. Operational Implementation of Prospective Genotyping for Personalized Medicine: The Design of the Vanderbilt PREDICT Project. Clin. Pharmacol. Ther. 2012, 92, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Pestian, J.; Spencer, M.; Matykiewicz, P.; Zhang, K.; Vinks, A.A.; Glauser, T. Personalizing Drug Selection Using Advanced Clinical Decision Support. Biomed. Inform. Insights 2009, 2, 19–29. [Google Scholar] [PubMed]
- Nutescu, E.A.; Drozda, K.; Bress, A.P.; Galanter, W.L.; Stevenson, J.; Stamos, T.D.; Desai, A.A.; Duarte, J.D.; Gordeuk, V.; Peace, D.; et al. Feasibility of Implementing a Comprehensive Warfarin Pharmacogenetics Service. Pharmacotherapy 2013. [Google Scholar] [CrossRef] [PubMed]
- Mega, J.L.; Hochholzer, W.; Frelinger, A.L., 3rd; Kluk, M.J.; Angiolillo, D.J.; Kereiakes, D.J.; Isserman, S.; Rogers, W.J.; Ruff, C.T.; Contant, C.; et al. Dosing clopidogrel based on CYP2C19 genotype and the effect on platelet reactivity in patients with stable cardiovascular disease. JAMA 2011, 306, 2221–2228. [Google Scholar] [CrossRef] [PubMed]
- Hall-Flavin, D.K.; Winner, J.G.; Allen, J.D.; Jordan, J.J.; Nesheim, R.S.; Snyder, K.A.; Drews, M.S.; Eisterhold, L.L.; Biernacka, J.M.; Mrazek, D.A. Using a pharmacogenomic algorithm to guide the treatment of depression. Transl. Psychiatry 2012, 2, e172. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, O.; Scott, S.A.; Ellis, S.B.; Overby, C.L.; Ludtke, A.; Hulot, J.-S.; Hall, J.; Chatani, K.; Myers, K.; Kannry, J.L.; et al. The CLIPMERGE PGx Program: Clinical implementation of personalized medicine through electronic health records and genomics-pharmacogenomics. Clin. Pharmacol. Ther. 2013, 94, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Dolan, M.E.; Maitland, M.L.; O’Donnell, P.H.; Nakamura, Y.; Cox, N.J.; Ratain, M.J. Institutional Profile: University of Chicago Center for Personalized Therapeutics: Research, education and implementation science. Pharmacogenomics 2013, 14, 1383–1387. [Google Scholar] [CrossRef] [PubMed]
- Bielinski, S.J.; Olson, J.E.; Pathak, J.; Weinshilboum, R.M.; Wang, L.; Lyke, K.J.; Ryu, E.; Targonski, P.V.; Van Norstrand, M.D.; Hathcock, M.A.; et al. Preemptive genotyping for personalized medicine: Design of the right drug, right dose, right time-using genomic data to individualize treatment protocol. Mayo Clin. Proc. 2014, 89, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Bell, G.C.; Crews, K.R.; Wilkinson, M.R.; Haidar, C.E.; Hicks, J.K.; Baker, D.K.; Kornegay, N.M.; Yang, W.; Cross, S.J.; Howard, S.C.; et al. Development and use of active clinical decision support for preemptive pharmacogenomics. J. Am. Med. Inform. Assoc. 2013. [Google Scholar] [CrossRef] [PubMed]
- Relling, M.V.; Klein, T.E. CPIC: Clinical Pharmacogenetics Implementation Consortium of the Pharmacogenomics Research Network. Clin. Pharmacol. Ther. 2011, 89, 464–467. [Google Scholar] [CrossRef] [PubMed]
- Whirl-Carrillo, M.; McDonagh, E.M.; Hebert, J.M.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Altman, R.B.; Klein, T.E. Pharmacogenomics knowledge for personalized medicine. Clin. Pharmacol. Ther. 2012, 92, 414–417. [Google Scholar] [CrossRef] [PubMed]
- PharmGKB. Available online: https://www.pharmgkb.org/ (accessed on 14 August 2017).
- CPIC. Available online: https://cpicpgx.org/ (accessed on 14 August 2017).
- Van Driest, S.L.; McGregor, T.L. Pharmacogenetics in clinical pediatrics: Challenges and strategies. Pers. Med. 2013, 10. [Google Scholar] [CrossRef] [PubMed]
- Wester, C.; Rebeiro, P.F.; Shavor, T.J.; Shepherd, B.E.; McGoy, S.L.; Daley, B.; Morrison, M.; Vermund, S.H.; Pettit, A.C. The 2013 HIV Continuum of Care in Tennessee: Progress Made, but Disparities Persist. Public Health Rep. 2016, 131, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Balyan, R.; Mecoli, M.; Venkatasubramanian, R.; Chidambaran, V.; Kamos, N.; Clay, S.; Moore, D.L.; Mavi, J.; Glover, C.D.; Szmuk, P.; et al. CYP2D6 pharmacogenetic and oxycodone pharmacokinetic association study in pediatric surgical patients. Pharmacogenomics 2017, 18, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Yue, Q.Y.; Svensson, J.O.; Alm, C.; Sjöqvist, F.; Säwe, J. Codeine O-demethylation co-segregates with polymorphic debrisoquine hydroxylation. Br. J. Clin. Pharmacol. 1989, 28, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.G.; Patel, A.; Howard, R.F. Pharmacogenetics of codeine metabolism in an urban population of children and its implications for analgesic reliability. Br. J. Anaesth. 2002, 89, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Koren, G.; Cairns, J.; Chitayat, D.; Gaedigk, A.; Leeder, S.J. Pharmacogenetics of morphine poisoning in a breastfed neonate of a codeine-prescribed mother. Lancet 2006, 368, 704. [Google Scholar] [CrossRef]
- Voronov, P.; Przybylo, H.J.; Jagannathan, N. Apnea in a child after oral codeine: A genetic variant—An ultra-rapid metabolizer. Paediatr. Anaesth. 2007, 17, 684–687. [Google Scholar] [CrossRef] [PubMed]
- Madadi, P.; Ross, C.J.D.; Hayden, M.R.; Carleton, B.C.; Gaedigk, A.; Leeder, J.S.; Koren, G. Pharmacogenetics of neonatal opioid toxicity following maternal use of codeine during breastfeeding: A case-control study. Clin. Pharmacol. Ther. 2009, 85, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Ciszkowski, C.; Madadi, P.; Phillips, M.S.; Lauwers, A.E.; Koren, G. Codeine, ultrarapid-metabolism genotype, and postoperative death. N. Engl. J. Med. 2009, 361, 827–828. [Google Scholar] [CrossRef] [PubMed]
- Ferreirós, N.; Dresen, S.; Hermanns-Clausen, M.; Auwaerter, V.; Thierauf, A.; Müller, C.; Hentschel, R.; Trittler, R.; Skopp, G.; Weinmann, W. Fatal and severe codeine intoxication in 3-year-old twins--interpretation of drug and metabolite concentrations. Int. J. Legal Med. 2009, 123, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Kelly, L.E.; Rieder, M.; van den Anker, J.; Malkin, B.; Ross, C.; Neely, M.N.; Carleton, B.; Hayden, M.R.; Madadi, P.; Koren, G. More codeine fatalities after tonsillectomy in North American children. Pediatrics 2012, 129, e1343–e1347. [Google Scholar] [CrossRef] [PubMed]
- Khetani, J.D.; Madadi, P.; Sommer, D.D.; Reddy, D.; Sistonen, J.; Ross, C.J.D.; Carleton, B.C.; Hayden, M.R.; Koren, G. Apnea and oxygen desaturations in children treated with opioids after adenotonsillectomy for obstructive sleep apnea syndrome: A prospective pilot study. Paediatr. Drugs 2012, 14, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Sistonen, J.; Madadi, P.; Ross, C.J.; Yazdanpanah, M.; Lee, J.W.; Landsmeer, M.L.A.; Nauta, M.; Carleton, B.C.; Koren, G.; Hayden, M.R. Prediction of codeine toxicity in infants and their mothers using a novel combination of maternal genetic markers. Clin. Pharmacol. Ther. 2012, 91, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Friedrichsdorf, S.J.; Nugent, A.P.; Strobl, A.Q. Codeine-associated pediatric deaths despite using recommended dosing guidelines: Three case reports. J. Opioid Manag. 2013, 9, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Prows, C.A.; Zhang, X.; Huth, M.M.; Zhang, K.; Saldaña, S.N.; Daraiseh, N.M.; Esslinger, H.R.; Freeman, E.; Greinwald, J.H.; Martin, L.J.; et al. Codeine-related adverse drug reactions in children following tonsillectomy: A prospective study. Laryngoscope 2014, 124, 1242–1250. [Google Scholar] [CrossRef] [PubMed]
- Gammal, R.S.; Crews, K.R.; Haidar, C.E.; Hoffman, J.M.; Baker, D.K.; Barker, P.J.; Estepp, J.H.; Pei, D.; Broeckel, U.; Wang, W.; et al. Pharmacogenetics for Safe Codeine Use in Sickle Cell Disease. Pediatrics 2016, 138, e20153479. [Google Scholar] [CrossRef] [PubMed]
- Kearns, G.L.; Leeder, J.S.; Gaedigk, A. Impact of the CYP2C19*17 allele on the pharmacokinetics of omeprazole and pantoprazole in children: Evidence for a differential effect. Drug Metab. Dispos. Biol. Fate Chem. 2010, 38, 894–897. [Google Scholar] [CrossRef] [PubMed]
- Lima, J.J.; Lang, J.E.; Mougey, E.B.; Blake, K.B.; Gong, Y.; Holbrook, J.T.; Wise, R.A.; Teague, W.G. Association of CYP2C19 polymorphisms and lansoprazole-associated respiratory adverse effects in children. J. Pediatr. 2013, 163, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Settin, A.; Abdalla, A.F.; Al-Hussaini, A.S.; El-Baz, R.; Galal, A. Cure rate of Helicobacter pylori infection in Egyptian children related to CYP2C19 gene polymorphism. Indian J. Gastroenterol. 2014, 33, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Lang, J.E.; Holbrook, J.T.; Mougey, E.B.; Wei, C.Y.; Wise, R.A.; Teague, W.G.; Lima, J.J. American Lung Association-Airways Clinical Research Centers Lansoprazole Is Associated with Worsening Asthma Control in Children with the CYP2C19 Poor Metabolizer Phenotype. Ann. Am. Thorac. Soc. 2015, 12, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Franciosi, J.P.; Mougey, E.B.; Williams, A.; Gomez-Suarez, R.A.; Thomas, C.; Creech, C.L.; George, K.; Corao, D.; Lima, J.J. Association Between CYP2C19*17 Alleles and pH Probe Testing Outcomes in Children With Symptomatic Gastroesophageal Reflux. J. Clin. Pharmacol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Clement, A.; Raney, J.J.; Wasserman, G.S.; Lowry, J.A. Chronic amitriptyline overdose in a child. Clin. Toxicol. (Phila. Pa.) 2012, 50, 431–434. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, B.; Olsson, G.; Reis, M.; Walinder, J.; Nordin, C.; Lundmark, J.; Scordo, M.G.; Dahl, M.L.; Bengtsson, F.; Ahlner, J. Enantioselective analysis of citalopram and metabolites in adolescents. Ther. Drug Monit. 2001, 23, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Rudberg, I.; Hendset, M.; Uthus, L.H.; Molden, E.; Refsum, H. Heterozygous mutation in CYP2C19 significantly increases the concentration/dose ratio of racemic citalopram and escitalopram (S-citalopram). Ther. Drug Monit. 2006, 28, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.R.; Najjar, F.; Rubin, L.H.; Guter, S.J.; Owley, T.; Mosconi, M.W.; Jacob, S.; Cook, E.H. Escitalopram pharmacogenetics: CYP2C19 relationships with dosing and clinical outcomes in autism spectrum disorder. Pharmacogenet. Genom. 2015. [Google Scholar] [CrossRef] [PubMed]
- Troost, P.W.; Lahuis, B.E.; Hermans, M.H.; Buitelaar, J.K.; van Engeland, H.; Scahill, L.; Minderaa, R.B.; Hoekstra, P.J. Prolactin release in children treated with risperidone: Impact and role of CYP2D6 metabolism. J. Clin. Psychopharmacol. 2007, 27, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Aman, M.G.; Vinks, A.A.; Remmerie, B.; Mannaert, E.; Ramadan, Y.; Masty, J.; Lindsay, R.L.; Malone, K. Plasma pharmacokinetic characteristics of risperidone and their relationship to saliva concentrations in children with psychiatric or neurodevelopmental disorders. Clin. Ther. 2007, 29, 1476–1486. [Google Scholar] [CrossRef] [PubMed]
- Correia, C.T.; Almeida, J.P.; Santos, P.E.; Sequeira, A.F.; Marques, C.E.; Miguel, T.S.; Abreu, R.L.; Oliveira, G.G.; Vicente, A.M. Pharmacogenetics of risperidone therapy in autism: Association analysis of eight candidate genes with drug efficacy and adverse drug reactions. Pharmacogenom. J. 2010, 10, 418–430. [Google Scholar] [CrossRef] [PubMed]
- Sherwin, C.M.T.; Saldaña, S.N.; Bies, R.R.; Aman, M.G.; Vinks, A.A. Population pharmacokinetic modeling of risperidone and 9-hydroxyrisperidone to estimate CYP2D6 subpopulations in children and adolescents. Ther. Drug Monit. 2012, 34, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Roke, Y.; van Harten, P.N.; Franke, B.; Galesloot, T.E.; Boot, A.M.; Buitelaar, J.K. The effect of the Taq1A variant in the dopamine D₂ receptor gene and common CYP2D6 alleles on prolactin levels in risperidone-treated boys. Pharmacogenet. Genom. 2013, 23, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Hendset, M.; Molden, E.; Knape, M.; Hermann, M. Serum concentrations of risperidone and aripiprazole in subgroups encoding CYP2D6 intermediate metabolizer phenotype. Ther. Drug Monit. 2014, 36, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Youngster, I.; Zachor, D.A.; Gabis, L.V.; Bar-Chaim, A.; Benveniste-Levkovitz, P.; Britzi, M.; Soback, S.; Ziv-Baran, T.; Berkovitch, M. CYP2D6 genotyping in paediatric patients with autism treated with risperidone: A preliminary cohort study. Dev. Med. Child Neurol. 2014, 56, 990–994. [Google Scholar] [CrossRef] [PubMed]
- Nussbaum, L.A.; Dumitraşcu, V.; Tudor, A.; Grădinaru, R.; Andreescu, N.; Puiu, M. Molecular study of weight gain related to atypical antipsychotics: Clinical implications of the CYP2D6 genotype. Rom. J. Morphol. Embryol. 2014, 55, 877–884. [Google Scholar] [PubMed]
- Dos Santos Júnior, A.; Henriques, T.B.; de Mello, M.P.; Ferreira Neto, A.P.; Paes, L.A.; Della Torre, O.H.; Sewaybricker, L.E.; Fontana, T.S.; Celeri, E.H.R.V.; Guerra Júnior, G.; et al. Hyperprolactinemia in Children and Adolescents with Use of Risperidone: Clinical and Molecular Genetics Aspects. J. Child Adolesc. Psychopharmacol. 2015, 25, 738–748. [Google Scholar] [CrossRef] [PubMed]
- Sukasem, C.; Hongkaew, Y.; Ngamsamut, N.; Puangpetch, A.; Vanwong, N.; Chamnanphon, M.; Chamkrachchangpada, B.; Sinrachatanant, A.; Limsila, P. Impact of Pharmacogenetic Markers of CYP2D6 and DRD2 on Prolactin Response in Risperidone-Treated Thai Children and Adolescents With Autism Spectrum Disorders. J. Clin. Psychopharmacol. 2016, 36, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Vanwong, N.; Ngamsamut, N.; Hongkaew, Y.; Nuntamool, N.; Puangpetch, A.; Chamnanphon, M.; Sinrachatanant, A.; Limsila, P.; Sukasem, C. Detection of CYP2D6 polymorphism using Luminex xTAG technology in autism spectrum disorder: CYP2D6 activity score and its association with risperidone levels. Drug Metab. Pharmacokinet. 2016, 31, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos-Júnior, A.; Henriques, T.B.; de Mello, M.P.; Della Torre, O.H.; Paes, L.A.; Ferreira-Neto, A.P.; Sewaybricker, L.E.; Fontana, T.S.; Celeri, E.H.R.V.; Guerra-Júnior, G.; et al. Pharmacogenetics of Risperidone and Cardiovascular Risk in Children and Adolescents. Int. J. Endocrinol. 2016, 2016, 5872423. [Google Scholar] [CrossRef] [PubMed]
- Mannheimer, B.; Haslemo, T.; Lindh, J.D.; Eliasson, E.; Molden, E. Risperidone and Venlafaxine Metabolic Ratios Strongly Predict a CYP2D6 Poor Metabolizing Genotype. Ther. Drug Monit. 2016, 38, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Medhasi, S.; Pinthong, D.; Pasomsub, E.; Vanwong, N.; Ngamsamut, N.; Puangpetch, A.; Chamnanphon, M.; Hongkaew, Y.; Pratoomwun, J.; Limsila, P.; et al. Pharmacogenomic Study Reveals New Variants of Drug Metabolizing Enzyme and Transporter Genes Associated with Steady-State Plasma Concentrations of Risperidone and 9-Hydroxyrisperidone in Thai Autism Spectrum Disorder Patients. Front. Pharmacol. 2016, 7, 475. [Google Scholar] [CrossRef] [PubMed]
- Vanwong, N.; Ngamsamut, N.; Medhasi, S.; Puangpetch, A.; Chamnanphon, M.; Tan-Kam, T.; Hongkaew, Y.; Limsila, P.; Sukasem, C. Impact of CYP2D6 Polymorphism on Steady-State Plasma Levels of Risperidone and 9-Hydroxyrisperidone in Thai Children and Adolescents with Autism Spectrum Disorder. J. Child Adolesc. Psychopharmacol. 2017, 27, 185–191. [Google Scholar] [CrossRef] [PubMed]
- DailyMed. ONDANSETRON—Ondansetron Hydrochloride Injection. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=e0050959-c14c-41b6-9a92-fadc5f6feff3 (accessed on 12 September 2017).
- DailyMed. ONDANSETRON—Ondansetron Hydrochloride Solution. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=ac3dfb81-a4c7-4147-9374-c234153b7c51 (accessed on 12 September 2017).
- Bell, G.C.; Caudle, K.E.; Whirl-Carrillo, M.; Gordon, R.J.; Hikino, K.; Prows, C.A.; Gaedigk, A.; Agundez, J.; Sadhasivam, S.; Klein, T.E.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2D6 genotype and use of ondansetron and tropisetron. Clin. Pharmacol. Ther. 2017, 102, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J.C.; Marsh, S.A.; Zaya, M.J.; Regina, K.J.; Divakaran, K.; Le, M.; Hines, R.N. Developmental changes in human liver CYP2D6 expression. Drug Metab. Dispos. 2008, 36, 1587–1593. [Google Scholar] [CrossRef] [PubMed]
- DailyMed. CODEINE SULFATE—Codeine Sulfate Tablet. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=fa3ed180-298a-4f9d-9d05-15182d7218bf (accessed on 12 September 2017).
- DailyMed. OXYCODONE HYDROCHLORIDE—Oxycodone Hydrochloride Solution. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=c193a56a-bb8f-476d-b1ec-789fd2aaef7e (accessed on 12 September 2017).
- DailyMed. Acetaminophen and Codeine Phosphate—Acetaminophen and Codeine Phosphate Liquid. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=7bca1d24-a317-44c4-8db2-68030eb961ed (accessed on 12 September 2017).
- Crews, K.R.; Gaedigk, A.; Dunnenberger, H.M.; Leeder, J.S.; Klein, T.E.; Caudle, K.E.; Haidar, C.E.; Shen, D.D.; Callaghan, J.T.; Sadhasivam, S.; et al. Clinical Pharmacogenetics Implementation Consortium Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450 2D6 genotype and codeine therapy: 2014 update. Clin. Pharmacol. Ther. 2014, 95, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Crews, K.R.; Gaedigk, A.; Dunnenberger, H.M.; Klein, T.E.; Shen, D.D.; Callaghan, J.T.; Kharasch, E.D.; Skaar, T.C. Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines for codeine therapy in the context of cytochrome P450 2D6 (CYP2D6) genotype. Clin. Pharmacol. Ther. 2012, 91, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Barron, J.J.; Tan, H.; Spalding, J.; Bakst, A.W.; Singer, J. Proton pump inhibitor utilization patterns in infants. J. Pediatr. Gastroenterol. Nutr. 2007, 45, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Vandenplas, Y.; Rudolph, C.D.; Di Lorenzo, C.; Hassall, E.; Liptak, G.; Mazur, L.; Sondheimer, J.; Staiano, A.; Thomson, M.; Veereman-Wauters, G.; et al. Pediatric gastroesophageal reflux clinical practice guidelines: Joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). J. Pediatr. Gastroenterol. Nutr. 2009, 49, 498–547. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, T.; Nakayama, K.; Yasuda, H.; Yoshida, M.; Asamura, T.; Ohrui, T.; Arai, H.; Araya, J.; Kuwano, K.; Yamaya, M. A randomized, single-blind study of lansoprazole for the prevention of exacerbations of chronic obstructive pulmonary disease in older patients. J. Am. Geriatr. Soc. 2009, 57, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- DailyMed. PRILOSEC—Omeprazole Magnesium Granule, Delayed Release. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=b6761f84-53ac-4745-a8c8-1e5427d7e179 (accessed on 12 September 2017).
- DailyMed. LANSOPRAZOLE—Lansoprazole Capsule, Delayed Release. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=fb26cbe4-d17a-41f7-8654-edebd8665f76 (accessed on 12 September 2017).
- DailyMed. DEXILANT—Dexlansoprazole Capsule, Delayed Release. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=9819f033-3bbe-442e-8e92-45fec77b237d (accessed on 12 September 2017).
- DailyMed. ESOMEPRAZOLE MAGNESIUM—Esomeprazole Magnesium Capsule, Delayed Release Pellets. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=eb8f8b81-d482-4b94-be87-c766f49e753f (accessed on 12 September 2017).
- DailyMed. PANTOPRAZOLE SODIUM—Pantoprazole Tablet, Delayed Release. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=f3ded82a-cf0d-4844-944a-75f9f9215ff0 (accessed on 12 September 2017).
- DailyMed. RABEPRAZOLE SODIUM—Rabeprazole Tablet, Delayed Release. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=951caefe-6e18-48ff-9567-beb545b09c25 (accessed on 12 September 2017).
- Proton Pump Inhibitors: Use in Pediatric Patients-ppi-pediatric-factsheet11-14.pdf. Available online: https://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/Pharmacy-Education-Materials/Downloads/ppi-pediatric-factsheet.pdf (accessed on 12 September 2017).
- Wedlund, P.J. The CYP2C19 enzyme polymorphism. Pharmacology 2000, 61, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, R.M.; Ohlsson, S.; Pedersen, R.S.; Mwinyi, J.; Ingelman-Sundberg, M.; Eliasson, E.; Bertilsson, L. Increased omeprazole metabolism in carriers of the CYP2C19*17 allele; a pharmacokinetic study in healthy volunteers. Br. J. Clin. Pharmacol. 2008, 65, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, S.J.; Begg, E.J. Pharmacogenetics, drug-metabolizing enzymes, and clinical practice. Pharmacol. Rev. 2006, 58, 521–590. [Google Scholar] [CrossRef] [PubMed]
- Shirai, N.; Furuta, T.; Moriyama, Y.; Okochi, H.; Kobayashi, K.; Takashima, M.; Xiao, F.; Kosuge, K.; Nakagawa, K.; Hanai, H.; et al. Effects of CYP2C19 genotypic differences in the metabolism of omeprazole and rabeprazole on intragastric pH. Aliment. Pharmacol. Ther. 2001, 15, 1929–1937. [Google Scholar] [CrossRef] [PubMed]
- Kearns, G.L.; Blumer, J.; Schexnayder, S.; James, L.P.; Adcock, K.G.; Reed, M.D.; Daniel, J.F.; Gaedigk, A.; Paul, J. Single-dose pharmacokinetics of oral and intravenous pantoprazole in children and adolescents. J. Clin. Pharmacol. 2008, 48, 1356–1365. [Google Scholar] [CrossRef] [PubMed]
- Knebel, W.; Tammara, B.; Udata, C.; Comer, G.; Gastonguay, M.R.; Meng, X. Population pharmacokinetic modeling of pantoprazole in pediatric patients from birth to 16 years. J. Clin. Pharmacol. 2011, 51, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Ward, R.M.; Tammara, B.; Sullivan, S.E.; Stewart, D.L.; Rath, N.; Meng, X.; Maguire, M.K.; Comer, G.M. Single-dose, multiple-dose, and population pharmacokinetics of pantoprazole in neonates and preterm infants with a clinical diagnosis of gastroesophageal reflux disease (GERD). Eur. J. Clin. Pharmacol. 2010, 66, 555–561. [Google Scholar] [CrossRef] [PubMed]
- DailyMed. SERTRALINE HYDROCHLORIDE—Sertraline Hydrochloride Solution. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=7f144b68-ae90-483c-b030-f6824662a734 (accessed on 12 September 2017).
- Rudberg, I.; Hermann, M.; Refsum, H.; Molden, E. Serum concentrations of sertraline and N-desmethyl sertraline in relation to CYP2C19 genotype in psychiatric patients. Eur. J. Clin. Pharmacol. 2008, 64, 1181–1188. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.; Liu, Z.Q.; Wang, W.; Chen, X.P.; Shu, Y.; He, N.; Zhou, H.H. Pharmacokinetics of sertraline in relation to genetic polymorphism of CYP2C19. Clin. Pharmacol. Ther. 2001, 70, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Van Nieuwerburgh, F.C.W.; Denys, D.A.J.P.; Westenberg, H.G.M.; Deforce, D.L.D. Response to serotonin reuptake inhibitors in OCD is not influenced by common CYP2D6 polymorphisms. Int. J. Psychiatry Clin. Pract. 2009, 13, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Brandl, E.J.; Tiwari, A.K.; Zhou, X.; Deluce, J.; Kennedy, J.L.; Müller, D.J.; Richter, M.A. Influence of CYP2D6 and CYP2C19 gene variants on antidepressant response in obsessive-compulsive disorder. Pharmacogenom. J. 2014, 14, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Grasmäder, K.; Verwohlt, P.L.; Rietschel, M.; Dragicevic, A.; Müller, M.; Hiemke, C.; Freymann, N.; Zobel, A.; Maier, W.; Rao, M.L. Impact of polymorphisms of cytochrome-P450 isoenzymes 2C9, 2C19 and 2D6 on plasma concentrations and clinical effects of antidepressants in a naturalistic clinical setting. Eur. J. Clin. Pharmacol. 2004, 60, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Lam, Y.W.F.; Gaedigk, A.; Ereshefsky, L.; Alfaro, C.L.; Simpson, J. CYP2D6 inhibition by selective serotonin reuptake inhibitors: Analysis of achievable steady-state plasma concentrations and the effect of ultrarapid metabolism at CYP2D6. Pharmacotherapy 2002, 22, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Hicks, J.K.; Bishop, J.R.; Sangkuhl, K.; Müller, D.J.; Ji, Y.; Leckband, S.G.; Leeder, J.S.; Graham, R.L.; Chiulli, D.L.; LLerena, A.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors. Clin. Pharmacol. Ther. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DailyMed. AMITRIPTYLINE HYDROCHLORIDE—Amitriptyline Hydrochloride Tablet, Film Coated. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=1e6d2c80-fbc8-444e-bdd3-6a91fe1b95bd (accessed on 12 September 2017).
- Hicks, J.K.; Swen, J.J.; Thorn, C.F.; Sangkuhl, K.; Kharasch, E.D.; Ellingrod, V.L.; Skaar, T.C.; Müller, D.J.; Gaedigk, A.; Stingl, J.C. Clinical Pharmacogenetics Implementation Consortium Clinical Pharmacogenetics Implementation Consortium guideline for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants. Clin. Pharmacol. Ther. 2013, 93, 402–408. [Google Scholar] [CrossRef] [PubMed]
- DailyMed. CITALOPRAM HYDROBROMIDE—Citalopram Tablet. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=a8e8fde2-8392-4d5b-902b-e2b9dd55a02d (accessed on 12 September 2017).
- DailyMed. ESCITALOPRAM—Escitalopram Oxalate Tablet, Film Coated. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=c7561244-68c9-6889-65b1-4ab8d1e09d2a (accessed on 12 September 2017).
- Amitai, M.; Kronenberg, S.; Carmel, M.; Michaelovsky, E.; Frisch, A.; Brent, D.; Apter, A.; Chen, A.; Weizman, A.; Fennig, S. Pharmacogenetics of citalopram-related side effects in children with depression and/or anxiety disorders. J. Neural Transm. 2016, 123, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.; Tybring, G.; Dahl, M.-L.; Lindh, J.D. Impact of cytochrome P450 2C19 polymorphisms on citalopram/escitalopram exposure: A systematic review and meta-analysis. Clin. Pharmacokinet. 2014, 53, 801–811. [Google Scholar] [CrossRef] [PubMed]
- Germann, D.; Kurylo, N.; Han, F. Risperidone. Profiles Drug Subst. Excip. Relat. Methodol. 2012, 37, 313–361. [Google Scholar] [CrossRef] [PubMed]
- Masri, B.; Salahpour, A.; Didriksen, M.; Ghisi, V.; Beaulieu, J.-M.; Gainetdinov, R.R.; Caron, M.G. Antagonism of dopamine D2 receptor/β-arrestin 2 interaction is a common property of clinically effective antipsychotics. Proc. Natl. Acad. Sci. USA 2008, 105, 13656–13661. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Takano, H.; Takahashi, H.; Arakawa, R.; Miyoshi, M.; Kodaka, F.; Okumura, M.; Otsuka, T.; Suhara, T. Effects of the antipsychotic risperidone on dopamine synthesis in human brain measured by positron emission tomography with l-[β-11C]DOPA: A stabilizing effect for dopaminergic neurotransmission? J. Neurosci. 2009, 29, 13730–13734. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Bourin, M.; Baker, G.B. Metabolism of risperidone to 9-hydroxyrisperidone by human cytochromes P450 2D6 and 3A4. Naunyn. Schmiedebergs Arch. Pharmacol. 1999, 359, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Dean, L. Risperidone Therapy and CYP2D6 Genotype. In Medical Genetics Summaries; Pratt, V., McLeod, H., Dean, L., Malheiro, A., Rubinstein, W., Eds.; National Center for Biotechnology Information (US): Bethesda, MD, USA, 2012. [Google Scholar]
- DailyMed. RISPERIDONE—Risperidone Tablet. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=1c3250f3-d291-4280-97d5-da3bb171e2b6 (accessed on 12 September 2017).
- Correll, C.U.; Penzner, J.B.; Parikh, U.H.; Mughal, T.; Javed, T.; Carbon, M.; Malhotra, A.K. Recognizing and monitoring adverse events of second-generation antipsychotics in children and adolescents. Child Adolesc. Psychiatr. Clin. N. Am. 2006, 15, 177–206. [Google Scholar] [CrossRef] [PubMed]
- De Leon, J.; Susce, M.T.; Pan, R.-M.; Fairchild, M.; Koch, W.H.; Wedlund, P.J. The CYP2D6 poor metabolizer phenotype may be associated with risperidone adverse drug reactions and discontinuation. J. Clin. Psychiatry 2005, 66, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.-F. Polymorphism of human cytochrome P450 2D6 and its clinical significance: Part I. Clin. Pharmacokinet. 2009, 48, 689–723. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.-F. Polymorphism of human cytochrome P450 2D6 and its clinical significance: Part II. Clin. Pharmacokinet. 2009, 48, 761–804. [Google Scholar] [CrossRef] [PubMed]
- Lane, H.-Y.; Liu, Y.-C.; Huang, C.-L.; Chang, Y.-C.; Wu, P.-L.; Lu, C.-T.; Chang, W.-H. Risperidone-related weight gain: Genetic and nongenetic predictors. J. Clin. Psychopharmacol. 2006, 26, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Novalbos, J.; López-Rodríguez, R.; Román, M.; Gallego-Sandín, S.; Ochoa, D.; Abad-Santos, F. Effects of CYP2D6 genotype on the pharmacokinetics, pharmacodynamics, and safety of risperidone in healthy volunteers. J. Clin. Psychopharmacol. 2010, 30, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Puangpetch, A.; Vanwong, N.; Nuntamool, N.; Hongkaew, Y.; Chamnanphon, M.; Sukasem, C. CYP2D6 polymorphisms and their influence on risperidone treatment. Pharmacogenom. Pers. Med. 2016, 9, 131–147. [Google Scholar] [CrossRef] [PubMed]
- Cabaleiro, T.; Ochoa, D.; López-Rodríguez, R.; Román, M.; Novalbos, J.; Ayuso, C.; Abad-Santos, F. Effect of polymorphisms on the pharmacokinetics, pharmacodynamics, and safety of risperidone in healthy volunteers. Hum. Psychopharmacol. 2014, 29, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Dodgen, T.M.; Eloff, A.; Mataboge, C.; Roos, L.J.L.; van Staden, W.C.W.; Pepper, M.S. Risperidone-associated adverse drug reactions and CYP2D6 polymorphisms in a South African cohort. Appl. Transl. Genom. 2015, 5, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Calarge, C.A.; Miller, D.D. Predictors of risperidone and 9-hydroxyrisperidone serum concentration in children and adolescents. J. Child Adolesc. Psychopharmacol. 2011, 21, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Green, D.J.; Mummaneni, P.; Kim, I.W.; Oh, J.M.; Pacanowski, M.; Burckart, G.J. Pharmacogenomic information in FDA-approved drug labels: Application to pediatric patients. Clin. Pharmacol. Ther. 2016, 99, 622–632. [Google Scholar] [CrossRef] [PubMed]
- Hines, R.N. Ontogeny of human hepatic cytochromes P450. J. Biochem. Mol. Toxicol. 2007, 21, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Relling, M.V.; Gardner, E.E.; Sandborn, W.J.; Schmiegelow, K.; Pui, C.-H.; Yee, S.W.; Stein, C.M.; Carrillo, M.; Evans, W.E.; Hicks, J.K.; et al. Clinical pharmacogenetics implementation consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing: 2013 update. Clin. Pharmacol. Ther. 2013, 93, 324–325. [Google Scholar] [CrossRef] [PubMed]
- Relling, M.V.; Gardner, E.E.; Sandborn, W.J.; Schmiegelow, K.; Pui, C.-H.; Yee, S.W.; Stein, C.M.; Carrillo, M.; Evans, W.E.; Klein, T.E. Clinical Pharmacogenetics Implementation Consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing. Clin. Pharmacol. Ther. 2011, 89, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Yu, G.; Li, G.-F.; Markowitz, J.S. Atomoxetine: A Review of Its Pharmacokinetics and Pharmacogenomics Relative to Drug Disposition. J. Child Adolesc. Psychopharmacol. 2016, 26, 314–326. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.A.; Caudle, K.E.; Gong, L.; Whirl-Carrillo, M.; Stein, C.M.; Scott, S.A.; Lee, M.T.; Gage, B.F.; Kimmel, S.E.; Perera, M.A.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Pharmacogenetics-Guided Warfarin Dosing: 2017 Update. Clin. Pharmacol. Ther. 2017, 102, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Stenner, S.P.; Doan, S.; Johnson, K.B.; Waitman, L.R.; Denny, J.C. MedEx: A medication information extraction system for clinical narratives. J. Am. Med. Inform. Assoc. 2010, 17, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Caudle, K.E.; Dunnenberger, H.M.; Freimuth, R.R.; Peterson, J.F.; Burlison, J.D.; Whirl-Carrillo, M.; Scott, S.A.; Rehm, H.L.; Williams, M.S.; Klein, T.E.; et al. Standardizing terms for clinical pharmacogenetic test results: Consensus terms from the Clinical Pharmacogenetics Implementation Consortium (CPIC). Genet. Med. 2017, 19, 215–223. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Rank | Drug | N Children Exposed | Median (IQR) Age at First Exposure (Years) | n (%) Male | n (%) White | n (%) Black/African American | n (%) Asian | n (%) Other | n (%) Unknown Race | n (%) Hispanic or Latino | n (%) Not Hispanic or Latino | n (%) Unknown Ethnicity |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | ondansetron | 114,059 | 6 (2–13) | 61,339 (53.8%) | 83,687 (73.4%) | 21,232 (18.6%) | 2188 (1.9%) | 1321 (1.2%) | 5631 (4.9%) | 11,161 (9.8%) | 98,732 (86.6%) | 4166 (3.7%) |
| 2 | oxycodone | 30,701 | 11 (4–16) | 16,330 (53.2%) | 22,696 (73.9%) | 4977 (16.2%) | 623 (2.0%) | 203 (0.7%) | 2202 (7.2%) | 2309 (7.5%) | 26,506 (86.3%) | 1886 (6.1%) |
| 3 | codeine | 21,086 | 4 (1–8) | 11,445 (54.3%) | 15,482 (73.4%) | 3928 (18.6%) | 445 (2.1%) | 254 (1.2%) | 977 (4.6%) | 1986 (9.4%) | 18,387 (87.2%) | 713 (3.4%) |
| 4 | omeprazole | 21,056 | 10 (4–15) | 10,355 (49.2%) | 15,531 (73.8%) | 2479 (11.8%) | 320 (1.5%) | 91 (0.4%) | 2635 (12.5%) | 1344 (6.4%) | 17,356 (82.4%) | 2356 (11.2%) |
| 5 | lansoprazole | 17,451 | 5 (0–11) | 9261 (53.1%) | 13,345 (76.5%) | 1663 (9.5%) | 217 (1.2%) | 132 (0.8%) | 2094 (12.0%) | 680 (3.9%) | 14,797 (84.8%) | 1974 (11.3%) |
| 6 | sertraline | 10,417 | 14 (10–16) | 4627 (44.4%) | 7931 (76.1%) | 1075 (10.3%) | 116 (1.1%) | 33 (0.3%) | 1262 (12.1%) | 379 (3.6%) | 8919 (85.6%) | 1119 (10.7%) |
| 7 | amitriptyline | 7918 | 13 (10–16) | 3020 (38.1%) | 5658 (71.5%) | 867 (10.9%) | 65 (0.8%) | 35 (0.4%) | 1293 (16.3%) | 340 (4.3%) | 6431 (81.2%) | 1147 (14.5%) |
| 8 | citalopram | 7528 | 13 (8–16) | 3751 (49.8%) | 5762 (76.5%) | 847 (11.3%) | 90 (1.2%) | 36 (0.5%) | 793 (10.5%) | 359 (4.8%) | 6489 (86.2%) | 680 (9.0%) |
| 9 | risperidone | 5485 | 11 (7–15) | 3793 (69.2%) | 3890 (70.9%) | 927 (16.9%) | 59 (1.1%) | 23 (0.4%) | 586 (10.7%) | 182 (3.3%) | 4767 (86.9%) | 536 (9.8%) |
| 10 | escitalopram | 5087 | 15 (12–17) | 2049 (40.3%) | 3990 (78.4%) | 396 (7.8%) | 73 (1.4%) | 22 (0.4%) | 606 (11.9%) | 181 (3.6%) | 4364 (85.8%) | 542 (10.7%) |
| 11 | atomoxetine | 3681 | 11 (8–14) | 2581 (70.1%) | 2776 (75.4%) | 350 (9.5%) | 29 (0.8%) | 16 (0.4%) | 510 (13.9%) | 86 (2.3%) | 3124 (84.9%) | 471 (12.8%) |
| 12 | paroxetine | 3445 | 7 (2–15) | 1641 (47.6%) | 2384 (69.2%) | 532 (15.4%) | 98 (2.8%) | 15 (0.4%) | 416 (12.1%) | 376 (10.9%) | 2786 (80.9%) | 283 (8.2%) |
| 13 | tramadol | 2731 | 14 (5–17) | 1228 (45.0%) | 2051 (75.1%) | 361 (13.2%) | 44 (1.6%) | 14 (0.5%) | 261 (9.6%) | 142 (5.2%) | 2366 (86.6%) | 223 (8.2%) |
| 14 | methadone | 2559 | 0 (0–4) | 1447 (56.5%) | 1901 (74.3%) | 376 (14.7%) | 32 (1.3%) | 22 (0.9%) | 228 (8.9%) | 184 (7.2%) | 2159 (84.4%) | 216 (8.4%) |
| 15 | tacrolimus | 2253 | 8 (3–13) | 1132 (50.2%) | 1434 (63.6%) | 440 (19.5%) | 67 (3.0%) | 15 (0.7%) | 297 (13.2%) | 170 (7.5%) | 1854 (82.3%) | 229 (10.2%) |
| 16 | nortriptyline | 2179 | 12 (8–16) | 864 (39.7%) | 1527 (70.1%) | 246 (11.3%) | 33 (1.5%) | 14 (0.6%) | 359 (16.5%) | 111 (5.1%) | 1754 (80.5%) | 314 (14.4%) |
| 17 | warfarin | 2091 | 9 (3–15) | 1107 (52.9%) | 1496 (71.5%) | 314 (15.0%) | 50 (2.4%) | 15 (0.7%) | 216 (10.3%) | 150 (7.2%) | 1804 (86.3%) | 137 (6.6%) |
| 18 | phenytoin | 1725 | 12 (3–16) | 980 (56.8%) | 1341 (77.7%) | 255 (14.8%) | 31 (1.8%) | 15 (0.9%) | 83 (4.8%) | 99 (5.7%) | 1542 (89.4%) | 84 (4.9%) |
| 19 | mirtazapine | 1578 | 12 (8–16) | 943 (59.8%) | 1155 (73.2%) | 211 (13.4%) | 26 (1.6%) | 4 (0.3%) | 182 (11.5%) | 72 (4.6%) | 1352 (85.7%) | 154 (9.8%) |
| 20 | venlafaxine | 1407 | 15 (8–17) | 558 (39.7%) | 1097 (78.0%) | 127 (9.0%) | 31 (2.2%) | 7 (0.5%) | 145 (10.3%) | 62 (4.4%) | 1232 (87.6%) | 113 (8.0%) |
| 21 | clopidogrel | 1131 | 7 (2–14) | 605 (53.5%) | 778 (68.8%) | 185 (16.4%) | 35 (3.1%) | 5 (0.4%) | 128 (11.3%) | 92 (8.1%) | 957 (84.6%) | 82 (7.3%) |
| 22 | imipramine | 877 | 11 (8–13) | 512 (58.4%) | 533 (60.8%) | 112 (12.8%) | 6 (0.7%) | 5 (0.6%) | 221 (25.2%) | 26 (3.0%) | 643 (73.3%) | 208 (23.7%) |
| 23 | celecoxib | 795 | 14 (6–16) | 351 (44.2%) | 605 (76.1%) | 85 (10.7%) | 14 (1.8%) | 1 (0.1%) | 90 (11.3%) | 45 (5.7%) | 678 (85.3%) | 72 (9.1%) |
| 24 | dexlansoprazole | 554 | 14 (9–16) | 264 (47.7%) | 444 (80.1%) | 49 (8.8%) | 13 (2.3%) | 2 (0.4%) | 46 (8.3%) | 35 (6.3%) | 480 (86.6%) | 39 (7.0%) |
| 25 | doxepin | 436 | 13 (6–17) | 194 (44.5%) | 294 (67.4%) | 69 (15.8%) | 8 (1.8%) | 1 (0.2%) | 64 (14.7%) | 19 (4.4%) | 356 (81.7%) | 61 (14.0%) |
| 26 | fluvoxamine | 414 | 13 (10–16) | 237 (57.2%) | 324 (78.3%) | 34 (8.2%) | 7 (1.7%) | 1 (0.2%) | 48 (11.6%) | 7 (1.7%) | 363 (87.7%) | 44 (10.6%) |
| 27 | voriconazole | 323 | 9 (3–15) | 183 (56.7%) | 247 (76.5%) | 44 (13.6%) | 8 (2.5%) | 1 (0.3%) | 23 (7.1%) | 25 (7.7%) | 280 (86.7%) | 18 (5.6%) |
| 28 | rabeprazole | 213 | 14 (8–16) | 96 (45.1%) | 161 (75.6%) | 22 (10.3%) | 1 (0.5%) | 3 (1.4%) | 26 (12.2%) | 10 (4.7%) | 180 (84.5%) | 23 (10.8%) |
| 29 | clomipramine | 188 | 13 (9–15) | 115 (61.2%) | 150 (79.8%) | 14 (7.4%) | 4 (2.1%) | 0 (0.0%) | 20 (10.6%) | 10 (5.3%) | 162 (86.2%) | 16 (8.5%) |
| 30 | tamoxifen | 83 | 11 (4–15) | 48 (57.8%) | 59 (71.1%) | 9 (10.8%) | 1 (1.2%) | 0 (0.0%) | 14 (16.9%) | 4 (4.8%) | 67 (80.7%) | 12 (14.5%) |
| 31 | nevirapine | 81 | 6 (0–12) | 40 (49.4%) | 27 (33.3%) | 40 (49.4%) | 0 (0.0%) | 1 (1.2%) | 13 (16.0%) | 4 (4.9%) | 66 (81.5%) | 11 (13.6%) |
| 32 | efavirenz | 56 | 13 (5–16) | 34 (60.7%) | 27 (48.2%) | 24 (42.9%) | 1 (1.8%) | 0 (0.0%) | 4 (7.1%) | 3 (5.4%) | 50 (89.3%) | 3 (5.4%) |
| 33 | quinidine | 56 | 10 (3–14) | 35 (62.5%) | 45 (80.4%) | 4 (7.1%) | 1 (1.8%) | 1 (1.8%) | 5 (8.9%) | 3 (5.4%) | 50 (89.3%) | 3 (5.4%) |
| 34 | desipramine | 49 | 13 (3–17) | 21 (42.9%) | 37 (75.5%) | 8 (16.3%) | 1 (2.0%) | 0 (0.0%) | 3 (6.1%) | 2 (4.1%) | 44 (89.8%) | 3 (6.1%) |
| 35 | trimipramine | 18 | 8 (2–13) | 11 (61.1%) | 13 (72.2%) | 2 (11.1%) | 0 (0.0%) | 0 (0.0%) | 3 (16.7%) | 0 (0.0%) | 15 (83.3%) | 3 (16.7%) |
| 36 | brexpiprazole | 13 | 16 (13–17) | 4 (30.8%) | 9 (69.2%) | 1 (7.7%) | 0 (0.0%) | 0 (0.0%) | 3 (23.1%) | 0 (0.0%) | 10 (76.9%) | 3 (23.1%) |
| 37 | tropisetron | 12 | 3 (1–10) | 7 (58.3%) | 10 (83.3%) | 1 (8.3%) | 0 (0.0%) | 0 (0.0%) | 1 (8.3%) | 0 (0.0%) | 11 (91.7%) | 1 (8.3%) |
| 38 | eliglustat | 6 | 11 (8–15) | 3 (50.0%) | 6 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 6 (100.0%) | 0 (0.0%) |
| 39 | protriptyline | 6 | 17 (14–17) | 1 (16.7%) | 4 (66.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (33.3%) | 0 (0.0%) | 4 (66.7%) | 2 (33.3%) |
| 40 | acenocoumarol | 3 | 13 (12–15) | 1 (33.3%) | 2 (66.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (33.3%) | 0 (0.0%) | 2 (66.7%) | 1 (33.3%) |
| 41 | phenprocoumon | 3 | 13 (12–15) | 1 (33.3%) | 2 (66.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (33.3%) | 0 (0.0%) | 2 (66.7%) | 1 (33.3%) |
| Drug | Gene | Variant(s) Assayed | Population | n | Significant Result | Results | Ref. |
|---|---|---|---|---|---|---|---|
| Oxycodone | CYP2D6 | *2–*11, *14, *15, *17–*20, *35, *40–*42, *44, duplication | 2–17-year-olds undergoing painful orthopedic, thoracic, urology and colorectal procedures | 30 | Yes | After oxycodone exposure, CYP2D6 normal metabolizers had greater oxymorphone exposure than poor or intermediate metabolizers | [18] |
| Codeine | CYP2D6 | CYP2D6 phenotype | 15–74-year-old healthy volunteers | 132 | Yes | After codeine administration, CYP2D6 poor metabolizers had lower formation of morphine versus normal metabolizers | [19] |
| Codeine | CYP2D6 | *2–*5, *9, *10, *17 | 3–12-year-olds undergoing adenotonsillectomy | 48 | Yes | After codeine administration, CYP2D6 poor metabolizers had reduced formation of morphine | [20] |
| Codeine | CYP2D6 | not stated | case report: breastfed neonate | 1 | -- | Fatal opioid poisoning in a breastfed neonate whose codeine-prescribed mother was a CYP2D6 ultra-rapid metabolizer | [21] |
| Codeine | CYP2D6 | not stated | case report: post-tonsillectomy codeine with apnea and brain injury | 1 | -- | 2-year-old child with codeine toxicity after tonsillectomy was CYP2D6*1/*2 | [22] |
| Codeine | CYP2D6 | not stated | mothers and infants with codeine exposure | 72 | Yes | Two of 17 mothers whose infants exhibited severe neonatal toxicity were CYP2D6 ultra-rapid metabolizers in combination with UGT2B7*2/*2 | [23] |
| Codeine | CYP2D6 | not stated | case report: fatality in child with adenotonsillectomy | 1 | -- | Death in a 2-year-old boy prescribed codeine for analgesia after adenotonsillectomy and with CYP2D6 ultra-rapid metabolizer phenotype | [24] |
| Codeine | CYP2D6 | *3–*6 | case report: fatality and respiratory failure in 3-year-old monozygotic twin brothers | 2 | -- | Death of one twin and respiratory failure with successful resuscitation of the other twin after administration of slow-release codeine cough medicine in CYP2D6 normal metabolizers | [25] |
| Codeine | CYP2D6 | not stated | case report: fatal or life-threatening codeine exposures after tosillectomy | 3 | -- | Two fatalities and one case of respiratory failure after post-tonsillectomy codeine exposure; one decedent was a CYP2D6 ultra-rapid metabolizer and the resuscitated child was a CYP2D6 normal metabolizer | [26] |
| Codeine | CYP2D6 | *2–*10, *12, *14 *17, *29, *41, duplication | 1–17-year-olds with obstructive sleep apnea syndrome who underwent adenotonsillectomy | 21 | No | CYP2D6 genotype did not predict change in the rate of desaturation and in the nadir oxygen saturation values | [27] |
| Codeine | CYP2D6 | *2–*10,*12, *14, *17, *29, *41, duplication | breastfeeding mothers using codeine and their infants | 111 | Yes | Maternal risk genotypes in CYP2D6 and ABCB1 were significantly associated with the adverse outcomes in infants | [28] |
| Codeine | CYP2D6 | not stated | case report: codeine related fatality | 3 | -- | One of the three cases of codeine fatality was a CYP2D6 normal metabolizer | [29] |
| Codeine | CYP2D6 | *2–*11, *14, *15, *17–*20, *35, *40–*42, *44, duplication | 6–15-year-olds undergoing tonsillectomy | 134 | Yes | Increased adverse drug reaction risk was associated with the presence of one or more full function CYP2D6 alleles | [30] |
| Codeine | CYP2D6 | Affymetrix DMET Plus GeneChip microarray, duplication | Patients with sickle cell disease | 830 | -- | None of the patients with an ultra-rapid or poor metabolizer CYP2D6 genotype were prescribed codeine | [31] |
| Omeprazole | CYP2C19 | *2–*8, *10, *12, *17 | 2–16-year-olds with therapeutic need for acid-modifying therapy | 23 | No | No relationship between CYP2C19 genotype and pharmacokinetic parameters (area under curve or clearance) | [32] |
| Lansoprazole | CYP2C19 | *2, *3, *8, *9, *17 | 6–17-year-olds with poor asthma control while treated with inhaled corticosteroids | 279 | Yes | Upper respiratory tract infections and strep throat were more frequent in CYP2C19 poor metabolizers than normal metabolizers or placebo | [33] |
| Lansoprazole | CYP2C19 | *1, *2, *3 | 0–18-year-olds with H. pylori infection | 100 | No | No significant difference in cure rates in CYP2C19 normal vs. poor metabolizers | [34] |
| Lansoprazole | CYP2C19 | *2, *3, *8–*10, *17 | 6–17-year-olds with poor asthma control while treated with inhaled corticosteroids | 279 | Yes | CYP2C19 poor metabolizers exposed to lansoprazole had worsening of asthma control | [35] |
| PPI | CYP2C19 | *2, *8, *17 | Children with gastroesophageal reflux refractory to PPI therapy | 74 | Yes | Increased acid exposure (lower intra-gastric pH) in CYP2C19 ultra-rapid metabolizers than non-ultra-rapid metabolizers | [36] |
| Amitriptyline | CYP2C19 | not stated | case report: 6-year-old child with amitriptyline overdose | 1 | -- | Patient survived a chronic 10-fold amitryptine overdose; genotyping revealed CYP2C19*1/*1 | [37] |
| Amitriptyline | CYP2D6 | not stated | case report: 6-year-old child with amitriptyline overdose | 1 | -- | Patient survived a chronic 10-fold amitryptine overdose; genotyping revealed CYP2D6*1/*41 | [37] |
| Citalopram | CYP2C19 | *2, *3 | 15–20-year-olds treated with citalopram for major depressive disorder or dysthymia | 19 | No | No difference in citalopram pharmacokinetics by CYP2C19 genotype | [38] |
| Citalopram | CYP2D6 | *2–*6, duplicaton | 15–20-year-olds treated with citalopram for major depressive disorder or dysthymia | 19 | No | No difference in citalopram pharmacokinetics by CYP2D6 genotype | [38] |
| Citalopram & Escitalopram | CYP2C19 | *2–*5 | 15–84-year-olds with citalopram or escitalopram therapeutic drug monitoring | 83 | Yes | CYP2C19 intermediate metabolizers had impaired metabolism of citalopram and S-citalopram compared to normal metabolizers | [39] |
| Escitalopram | CYP2C19 | *2,*3,*17 | 4–45-year-olds with ASD | 89 | No | No significant difference in citalopram dose by CYP2C19 metabolizer status | [40] |
| Risperidone | CYP2D6 | *3–*7, duplication | 5–17-year-olds with pervasive developmental disorder | 25 | Yes | Serum prolactin level was positively correlated with CYP2D6 function | [41] |
| Risperidone | CYP2D6 | *3–*5, duplication | 4–15-year-olds treated with risperidone for psychiatric or neurodevelopmental conditions | 19 | No | In pharmacokinetic analysis, one outlier identified was found to be a CYP2D6 poor metabolizer | [42] |
| Risperidone | CYP2D6 | *3–*6, duplication | 3–21-year-olds with ASD | 45 | Yes | CYP2D6 polymorphisms were associated with risperidone-induced increase in body mass index or waist circumference | [43] |
| Risperidone | CYP2D6 | *2–*11, *14, *15, *17–*20, *40–*42, duplication | 3–18-year-olds treated with risperidone for a neuropsychiatric disorder | 28 | No | Clearance estimates for a 1-compartment mixture model were highest for CYP2D6 normal metabolizers and lowest for poor metabolizers | [44] |
| Risperidone | CYP2D6 | *3, *4, *5, *6, duplication | 10–19-year-old males with ASD or disruptive behavior disorders | 47 | No | No statistically signifant difference in prolactin level by CYP2D6 functional status | [45] |
| Risperidone | CYP2D6 | *3, *4, *5, *6, *9, *10, *41 | 8–89-year-olds with risperidone TDM | 190 | Yes | Higher risperidone serum concentration in those with reduced CYP2D6 function | [46] |
| Risperidone | CYP2D6 | *2–*11, *14, *15, *17–*20, *25, *26, *29, *30, *31, *35–*37, *40, *41, *43, *52, duplication | 3–18-year-olds with ASD or pervasive developmental disorders | 40 | Yes | Higher risperidone plasma concentrations and risperidone:9-hydroxyrisperidone ratio in CYP2D6 poor metabolizers, but no significant association between the CYP2D6 function and clinical response or adverse effects | [47] |
| Risperidone | CYP2D6 | *4 | 9–20-year-olds with schizophrenia or bipolar disorder | 81 | Yes | Significantly higher weight gain in those with CYP2D6*4 | [48] |
| Risperidone | CYP2D6 | *10 | 8–20-year-olds treated with risperidone for mental or behavioral disorder | 120 | No | No significant association between plasma prolactin levels and CYP2D6*10 allele | [49] |
| Risperidone | CYP2D6 | *4, *5, *10, *41 | 3–19-year-olds with ASD | 147 | No | No significant correlation of prolactin levels and CYP2D6 genotype | [50] |
| Risperidone | CYP2D6 | *2–*11, *15, *29, *33, *41, duplication | 3–20-year-olds with ASD | 84 | Yes | Higher risperidone plasma concentration risperidone: 9-hydroxyrisperidone ratio among those with reduced CYP2D6 function | [51] |
| Risperidone | CYP2D6 | *10 | 8–20-year-olds treated with risperidone for mental and behavioral disorders | 120 | Yes | Obese/overweight and hypertension were associated with CYP2D6*10 | [52] |
| Risperidone | CYP2D6 | *3–*6, *9, *10, *41, duplication | 9–93-year-olds with risperidone TDM | 425 | Yes | Risperidone: 9-hydroxyrisperidone concentration ratio correlated with CYP2D6 function | [53] |
| Risperidone | CYP2D6 | Affymetrix DMET Plus GeneChip microarray | Children with ASD (median age 8.8 (IQR 3.4–18.6) years) | 102 | Yes | CYP2D6 variants were associated with risperidone plasma concentration and the risperidone: 9-hydroxyrisperidone ratio | [54] |
| Risperidone | CYP2D6 | *4, *5, *10, *41 | Children with ASD (median age 10 (IQR 7–12.15) years) | 97 | Yes | Plasma levels of risperidone were significantly higher in individuals with decreased CYP2D6 function | [55] |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aka, I.; Bernal, C.J.; Carroll, R.; Maxwell-Horn, A.; Oshikoya, K.A.; Van Driest, S.L. Clinical Pharmacogenetics of Cytochrome P450-Associated Drugs in Children. J. Pers. Med. 2017, 7, 14. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm7040014
Aka I, Bernal CJ, Carroll R, Maxwell-Horn A, Oshikoya KA, Van Driest SL. Clinical Pharmacogenetics of Cytochrome P450-Associated Drugs in Children. Journal of Personalized Medicine. 2017; 7(4):14. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm7040014
Chicago/Turabian StyleAka, Ida, Christiana J. Bernal, Robert Carroll, Angela Maxwell-Horn, Kazeem A. Oshikoya, and Sara L. Van Driest. 2017. "Clinical Pharmacogenetics of Cytochrome P450-Associated Drugs in Children" Journal of Personalized Medicine 7, no. 4: 14. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm7040014